
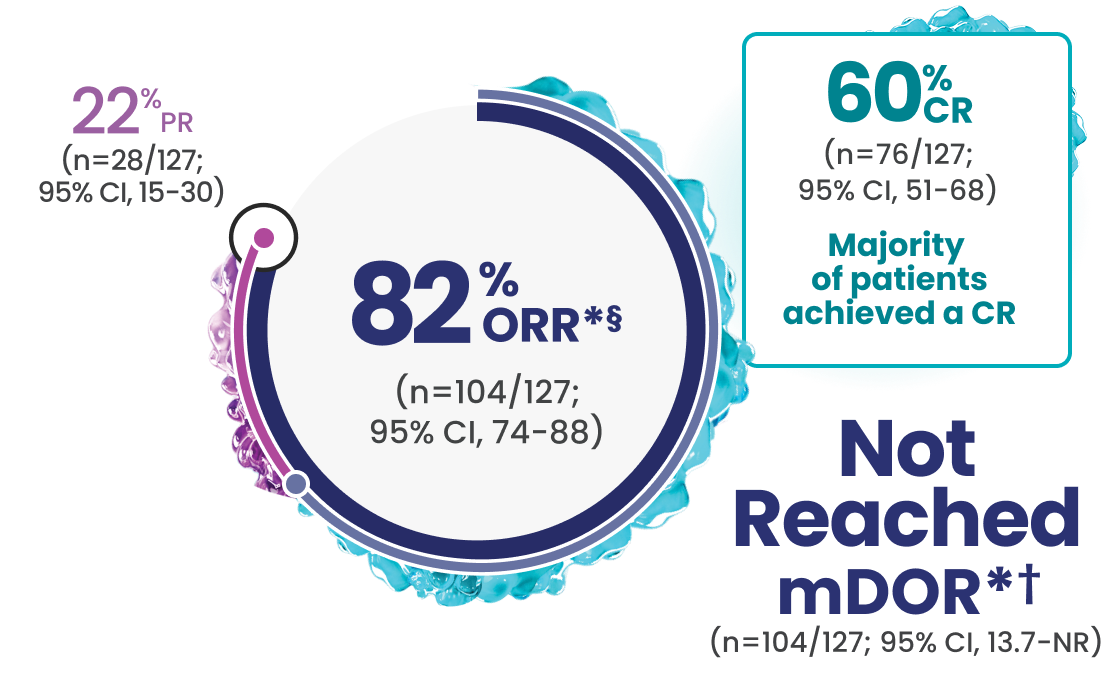
Even with a high enrollment of patients with difficult-to-treat disease,‡ 60% CR was observed in EPCORE® NHL-11-4
Rapid response1
- In responders (n=104), the median time to first response was 1.4 months (range: 1-3 months)*
In a prespecified analysis of complete responders (n=76), the median time to complete response was 1.5 months (range: 1.2-11.1).5*
*Efficacy results determined by Lugano criteria (2014) as assessed by Independent Review Committee (IRC).1
†Based on Kaplan-Meier estimate. The median follow-up for DOR was 14.8 months.5
‡Difficult-to-treat disease characteristics included age >65, double refractory, refractory to ≥2 consecutive lines of antilymphoma therapy, and POD24.1-4
§Median study follow-up was 17.4 months.6
The efficacy results of the 86 patients who received the recommended 3-step up dosage schedule in the EPCORE® NHL-1 dose optimization cohort were comparable to the primary efficacy endpoints.1‖
- Investigator-assessed efficacy outcomes6,7:
- ORR: 86% (n=74/86; 95% Cl, 76.9-92.6)
- CR: 64% (n=55/86; 95% Cl, 52.9-74.0)
- PR: 22% (n=19/86)
‖Median study follow-up for the dose optimization cohort was 5.7 months.6
Manageable Safety Profile1
- With the 3-step up dosage schedule:
- No grade ≥3 CRS events were observed; CRS occurred in 49% of patients (45% grade 1; 9% grade 2)¶
- Warnings and precautions include CRS, ICANS, infections, cytopenias, and embryo-fetal toxicity
- Most common (≥20%) adverse reactions were CRS, injection site reactions, fatigue, musculoskeletal pain, fever, diarrhea, COVID-19, rash, and abdominal pain
Please see full Important Safety Information, including Boxed Warnings.
¶In 86 patients who received EPKINLY following the recommended 3-step up dosage schedule.
OFF-THE-SHELF SUBCUTANEOUS
OUTPATIENT ADMINISTRATION1
Hospitalization is not required to administer EPKINLY for R/R FL—assess each patient
- For patients with FL, assess whether hospitalization or outpatient monitoring for the first 48 mg dose is appropriate based on comorbidities or other situational factors
- During outpatient monitoring after the first 48 mg dose, patients should remain in proximity to a healthcare facility that can assess and manage CRS
- EPKINLY should only be administered by a qualified HCP with appropriate medical support to manage severe reactions such as CRS and ICANS
- Due to the risk of CRS and ICANS, monitor all patients for signs and symptoms
- Hospitalization may be needed to manage some adverse reactions
NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) Recommended
The NCCN Guidelines® recommend epcoritamab-bysp (EPKINLY) as an NCCN Category 2A preferred treatment option after 2 or more lines of systemic therapy for patients with relapsed or refractory follicular lymphoma.8#
NCCN makes no warranties of any kind whatsoever regarding their content, use or application and disclaims any responsibility for their application or use in any way.
#See NCCN Guidelines for the NCCN definitions of Categories of Preference and Categories of Evidence and Consensus.
2L=second line; 3L=third line; AR=adverse reaction; CI=confidence interval; CR=complete response; CRS=cytokine release syndrome; DOR=duration of response; FL=follicular lymphoma; ICANS=immune effector cell–associated neurotoxicity syndrome; mDOR=median duration of response; NCCN=National Comprehensive Cancer Network® (NCCN®); NHL=non-Hodgkin lymphoma; NR=not reached; ORR=overall response rate; POD24=progression of disease within 24 months; PR=partial response; R/R=relapsed/refractory.